
Case 24: Management of a Common Bile Duct Stone in a 55-Year-Old Female
A 55-year-old female presented to the emergency department with a two-day history of sharp, intermittent right upper quadrant (RUQ) pain that radiated to her back. She also noticed yellowing of her eyes (jaundice) and nausea but denied vomiting, fever or changes in bowel habits. She has a history of gallstones diagnosed two years ago, which were incidentally seen on transabdominal ultrasound and were asymptomatic. She is hemodynamically stable with mild scleral icterus. On examination, there is tenderness in the RUQ with a positive Murphy’s sign. There is no rebound tenderness or guarding. Her liver enzymes are elevated with evidence of biliary obstruction: aspartate aminotransferase (AST): 145 U/L (normal 10-40), alanine aminotransferase (ALT): 160 U/L (normal 7-56), alkaline phosphatase (ALP): 350 U/L (normal 40-129), and total bilirubin: 3.8 mg/dL (normal 0.1-1.2), with a direct bilirubin of 2.5 mg/dL (normal 0-0.3). Amylase and lipase were within normal limits. She underwent a transabdominal ultrasound, which showed gallstones with common bile duct (CBD) dilation to 9 mm, but no stones were directly visualized in the duct. Magnetic resonance cholangiopancreatography (MRCP) was then performed. This confirmed an 8 mm stone in the distal common bile duct with mild intrahepatic and extrahepatic biliary ductal dilatation (Image 1).
Image 1: MRCP showing distal CBD stone

Image from the personal library of Sarah Enslin
What is the appropriate management of this patient’s condition?
- Endoscopic ultrasound
- Surgical consultation for common bile duct exploration
- Endoscopic retrograde cholangiopancreatography (ERCP)
- Supportive management
The correct answer is C, endoscopic retrograde cholangiopancreatography (ERCP)
Practice Pearls
Epidemiology and Risk Factors
- CBD stones are a common complication in patients with gallstones, affecting up to 15% of this population.1
- Risk factors include advanced age, history of gallstones, prior cholecystectomy and anatomical abnormalities of the biliary system.1
Complications
- Left untreated, CBD stones can lead to serious complications, such as cholangitis, gallstone pancreatitis and secondary biliary cirrhosis.1
Diagnosis
- Abdominal ultrasound is an excellent first-line imaging test, especially for evaluating biliary dilation, but it may not detect smaller or noncalcified stones.1,2
- MRCP is highly sensitive for confirming the diagnosis of CBD stones and identifying alternative causes of biliary obstruction.1,2
- Elevated liver function tests (LFTs), particularly ALT, AST, ALP and bilirubin, support the diagnosis. However, LFT normalization does not rule out CBD stones.2
- A differential diagnosis of biliary obstruction includes biliary strictures (benign and malignant), cholangiocarcinoma, Mirizzi syndrome, choledochal cysts, pancreatic head malignancy and primary sclerosing cholangitis.
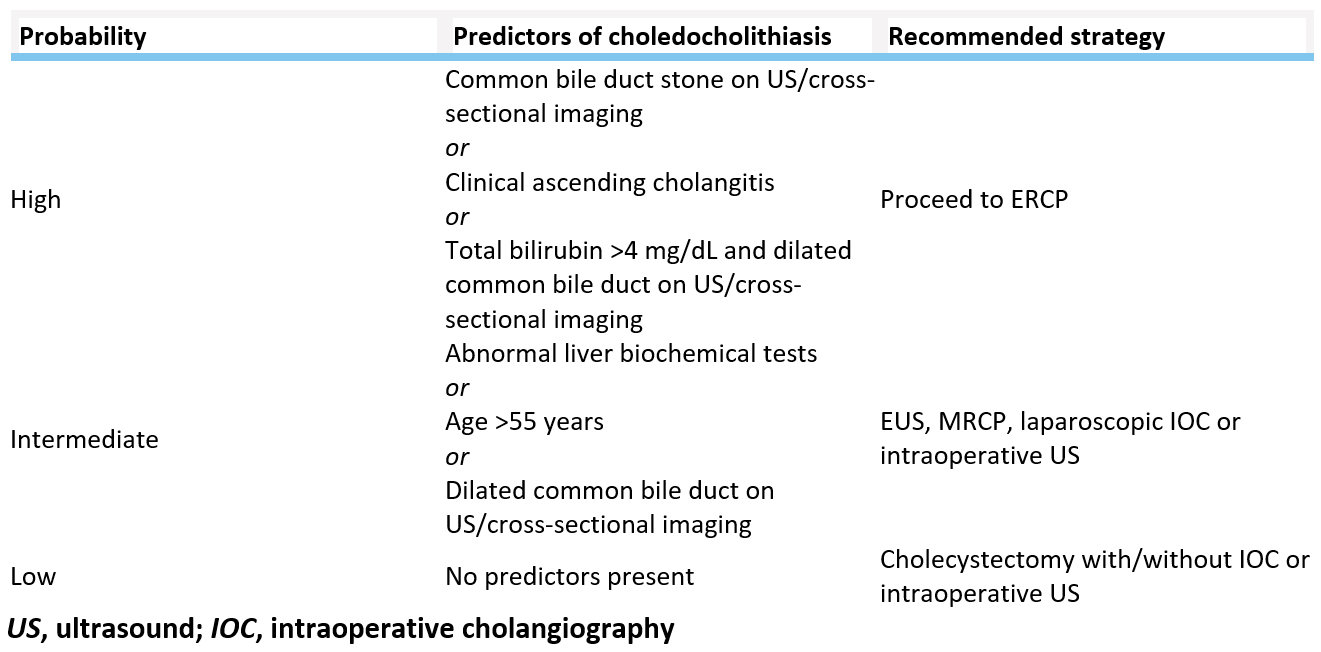
- Image 2 provides risk stratification of choledocholithiasis in patients with established cholelithiasis and the next best steps in management.2
Image 2: Table on proposed strategy to assign risk of choledocholithiasis and manage patients with symptomatic cholelithiasis based on clinical predictors
Management
- ERCP with stone removal is the standard treatment for CBD stones. Balloon or basket extraction is commonly performed during the procedure.1,2
- A temporary plastic biliary stent may be placed after ERCP to ensure bile duct patency in certain cases. These stents are typically removed or exchanged within four to six weeks.
- For patients with cholangitis or gallstone pancreatitis, early ERCP within 24 to 48 hours is recommended.2
- To prevent recurrence, elective cholecystectomy is recommended for most patients.2
- For patients who are clinically stable after ERCP, early cholecystectomy during the same hospitalization is preferred to reduce the risk of recurrence, particularly in those presenting with gallstone pancreatitis.1
- Lifestyle modifications, including maintaining a healthy weight and managing dyslipidemia, may reduce the risk of recurrent gallstones.
- Ursodeoxycholic acid has limited evidence in preventing the recurrence of CBD stones but may be considered in select high-risk populations.
Role of Advanced Practice Providers
Advanced practice providers play a crucial role in managing these cases in the following ways:
- Recognizing key symptoms such as RUQ pain and jaundice
- Ordering appropriate diagnostic tests, including imaging and liver function studies
- Collaborating with gastroenterologists and surgeons for definitive care
- Educating patients on the importance of follow-up and preventive measures, such as cholecystectomy
References
- Azeem N, Arain MA, Freeman ML. Choledocholithiasis: Clinical manifestations, diagnosis, and management. UpToDate. Updated February 28, 2023. https://www.uptodate.com/contents/choledocholithiasis-clinical-manifestations-diagnosis-and-management
- ASGE Standards of Practice Committee, Buxbaum JL, Abbas Fehmi SM, Sultan S, et al. ASGE guideline on the role of endoscopy in the evaluation and management of choledocholithiasis. Gastrointest Endosc. 2019;89:1075-1105.e15.
 Inessa Khaykis, MD, FASGE, is a clinical professor of medicine at New York University Grossman School of Medicine and a managing partner of Vanguard Gastroenterology Group in New York City. She is on the management board of Kips Bay Endoscopy Center. Dr. Khaykis is an alumnus of the ASGE Leadership Education and Development (LEAD) Program and the former chair of the ASGE Practice Operations Committee. She currently serves on the ASGE Practice Operations Committee and the ASGE APP Committee.
Inessa Khaykis, MD, FASGE, is a clinical professor of medicine at New York University Grossman School of Medicine and a managing partner of Vanguard Gastroenterology Group in New York City. She is on the management board of Kips Bay Endoscopy Center. Dr. Khaykis is an alumnus of the ASGE Leadership Education and Development (LEAD) Program and the former chair of the ASGE Practice Operations Committee. She currently serves on the ASGE Practice Operations Committee and the ASGE APP Committee.
 Sarah Enslin, PA-C, is a physician assistant at the University of Rochester Medical Center in Rochester, NY, with over 10 years of experience as a practicing PA in GI. Sarah serves on several national GI committees and is a former member of the ASGE Practice Operations Committee and a current member of the ASGE APP Committee.
Sarah Enslin, PA-C, is a physician assistant at the University of Rochester Medical Center in Rochester, NY, with over 10 years of experience as a practicing PA in GI. Sarah serves on several national GI committees and is a former member of the ASGE Practice Operations Committee and a current member of the ASGE APP Committee.
 Katelyn Cookson, PA-C, is a physician assistant, specializing in gastroenterology at UCHealth Digestive Health Center, and an instructor at the University of Colorado Anschutz Medical Campus. Katelyn serves as co-chair of the ASGE APP Committee.
Katelyn Cookson, PA-C, is a physician assistant, specializing in gastroenterology at UCHealth Digestive Health Center, and an instructor at the University of Colorado Anschutz Medical Campus. Katelyn serves as co-chair of the ASGE APP Committee.