
A 46-year-old man with poorly controlled diabetes presents with a two day history of severe epigastric pain that radiates to his back with associated nausea and vomiting.
Patient denies any alcohol or tobacco use. Patient denies taking any medications other than insulin which he ran out of last month.
On physical exam, the patient is tender to palpation to epigastric and LUQ. HR 115, BP 156/60. He is afebrile. Labs demonstrate lipase >2000 U/L, normal liver enzymes, calcium 9.3 mg/dL, triglycerides 1250 mg/dL. RUQ ultrasound demonstrates normal appearing gallbladder, CBD measuring 3 mm, edematous appearing pancreas consistent with pancreatitis.
What is the most likely etiology for his pancreatitis?
- Gallstones
- Alcohol
- Hypertriglycerides
- Hypercalcemia
Show Answer
The correct answer is C, Hypertriglycerides
PRACTICE PEARLS
Epidemiology
Diagnosis
- Diagnosis of acute pancreatitis is made by identifying 2 of the 3 following criteria: abdominal pain consistent with the disease, serum amylase, and/or lipase greater than 3 times the upper limit of normal, and/or characteristic findings from abdominal imaging 2
- In the absence of gallstones and/or significant alcohol history, serum triglycerides should be obtained. Serum triglyceride levels >500 mg/dL are required for HTG to be considered the etiology of acute pancreatitis. 1, 2
Management
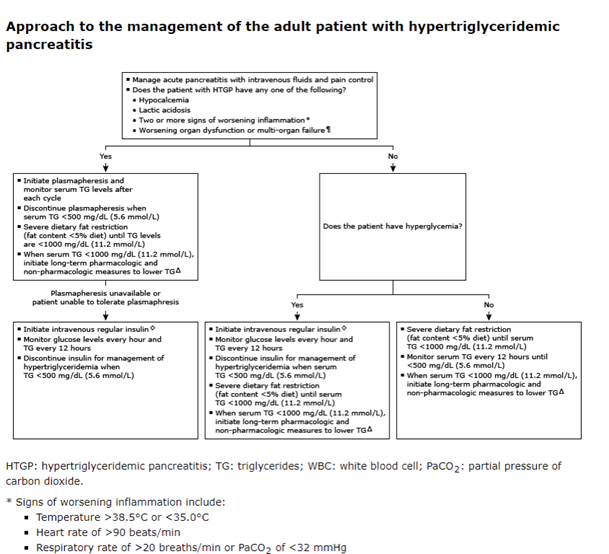
- Moderately aggressive fluid resuscitation with lactated ringers is preferred; consider additional fluid bolus for patients with hypovolemia. 2
- Supportive care with pain control and antiemetics
- Monitor serum triglycerides every 12 hours until <500 mg/dL
- Specific therapy for HTG includes IV insulin infusion to rapidly decrease triglyceride levels or plasmapheresis in patients with worrisome features such as worsening systemic inflammation, organ dysfunction or multi organ failure, or lactic acidosis. 3
- No role for prophylactic antibiotics 2
- Severe dietary fat restriction if serum triglycerides are >1000 mg/dL; for moderate to moderately severe pancreatitis consider enteral nutrition via NG tube 2
- Once triglycerides are <500 mg/dL, patients will require long term therapy to prevent recurrent pancreatitis which consists of both pharmacologic therapy and non-pharmacologic interventions such as dietary modifications, weight loss, and exercise 2
Role of NP
- All aspects of care in acute HTG induced pancreatitis, including diagnosis, work-up, risk stratification, and multidisciplinary management
- Guide long-term management strategies and secondary prevention, including lipid management, lifestyle modification, and multidisciplinary care coordination with endocrinology, dietitians, and PCPs
- Patient education on early recognition of symptoms, adherence to a low fat diet and lifestyle modifications, compliance with pharmacologic therapy, and long-term management including triglyceride management and comorbidity control
- Hypertriglyceridemia (HTG) is the third most common cause of pancreatitis causing 1-30% of all cases of acute pancreatitis and up to 50% of all cases during pregnancy 1
- Patient with HTG induced pancreatitis often are younger, predominantly male and have a history of obesity and/or diabetes 1
- The degree of HTG is associated with the severity of acute pancreatitis 1
- Risk of acute pancreatitis increases with the number of prior episodes of pancreatitis 1
REFERENCES
- Gelrud A. Hypertriglyceridemia-induced acute pancreatitis. In: UpToDate, Connor RF (Ed), Wolters Kluwer. Accessed on November 9, 2025
- Tenner S, Vege SS, Sheth SG, Sauer B, Yang A, Conwell DL, Yadlapati RH, Gardner TB. American College of Gastroenterology Guidelines: Management of Acute Pancreatitis. Am J Gastroenterol. 2024 Mar 1;119(3):419-437. doi: 10.14309/ajg.0000000000002645. Epub 2023 Nov 7. PMID: 38857482.
- Allison L. Yang, Julia McNabb-Baltar, Hypertriglyceridemia and acute pancreatitis, Pancreatology, Volume 20, Issue 5, 2020, Pages 795-800, ISSN 1424-3903, https://doi.org/10.1016/j.pan.2020.06.005. (https://www.sciencedirect.com/science/article/pii/S1424390320301988)
Authors

Janelle DeFilippis, APN-BC is a board certified Acute Care Nurse Practitioner at Rockford Gastroenterology Associates specializing in the care of hospitalized patients with gastroenterological problems at OSF Saint Anthony Hospital. She received her BSN degree from Saint Anthony College of Nursing and earned her MSN and Acute Care Certification from University of Illinois in Chicago.

Jennifer Ward, APN-BC is a board certified Nurse Practitioner at Rockford Gastroenterology Associates, specializing in the care of hospitalized patients with gastroenterological problems at OSF Saint Anthony’s Hospital. She received her BSN degree from Saint Anthony College of Nursing and earned her MSN from Northern Illinois University.