
A 62-year-old, Caucasian male presents for a 6-month history of nausea and abdominal discomfort. He reports a 10-year history of heartburn at least 4 times per week, taking calcium carbonate for relief. He has never had an upper endoscopy. His BMI is 31. He has a family history of Barrett’s esophagus.
Screening for Barrett’s esophagus is suggested for patients with chronic GERD symptoms and 3 or more additional risk factors for Barrett’s esophagus except?
- Age >50 years
- Caucasian race
- Obesity
- Tobacco smoking
- Current or history of alcohol use
Show Answer
The correct answer is E, current or history of alcohol use.
PRACTICE PEARLS
Screening
- Screening for Barrett’s esophagus is recommended in patients with a history of chronic gastroesophageal reflux disease symptoms and 3 or more additional risk factors for Barrett’s esophagus including male sex, age greater than 50 years, white race, tobacco smoking, obesity, family history of Barrett’s esophagus or esophageal adenocarcinoma in a first-degree relative.1
- Counsel patients on benefits and risks, consider financial and time considerations as well as patient comorbidities.1
Diagnosis
- The diagnosis of Barrett’s esophagus requires extension of columnar epithelium in the tubular esophagus greater than or equal to 1 cm above the gastroesophageal junction and histological evidence of specialized intestinal metaplasia.1
- Barrett’s esophagus is best described by using the Prague criteria that includes both the circumferential and maximal (C-M) extent of the columnar epithelium.4
- At least 8 biopsies from the Barrett’s segment are required.1
- Careful examination for mucosal irregularities (lumps or bumps harboring nests of dysplasia or cancer)
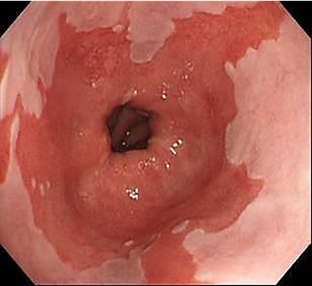
Image from personal library of Sarel Myburgh
Gastroesophageal reflux disease
- Patients with grade C or D esophagitis require follow-up endoscopy in 2-3 months after twice daily high-dose PPI therapy.2-3
- It is estimated that up to 15% of patients with erosive esophagitis will have Barrett’s found at endoscopy after healing erosive esophagitis.3
- Patients with Barrett’s should be on at least once daily proton pump inhibitor (PPI) if they have no allergy or contraindication to PPI.1
- Continue aggressive lifestyle modifications for gastroesophageal reflux disease including head of bed elevation, weight loss for those who are overweight or obese, avoiding meals 2-3 hours before bedtime and smoking cessation.2
Management
- Endoscopic surveillance is performed at the intervals based on the degree of dysplasia noted.1
- Segments of ≥3 cm surveyed on 3-year interval while segments of < 3 cm surveyed on 5-year interval.1
- Endoscopic surveillance should employ four-quadrant biopsies at 2 cm intervals in patients without dysplasia and 1 cm intervals in patients with prior dysplasia.1
- Barrett’s with dysplasia, review pathology slides by expert pathologist as there is considerable interobserver variability and it is more difficult to interpret low grade dysplasia and indefinite for dysplasia.1
- Endoscopic eradication is recommended in patients with low-grade and high-grade dysplasia to prevent progression to esophageal adenocarcinoma.1
- Modalities for endoscopic eradication include endoscopic mucosal resection, radiofrequency ablation and cryoablation.1
- The goal of endoscopic therapy is complete remission of dysplasia and finally complete remission of intestinal metaplasia.1
- Consider referral to center of expertise as treatment at high-volume centers is associated with reduced risk of recurrence.5
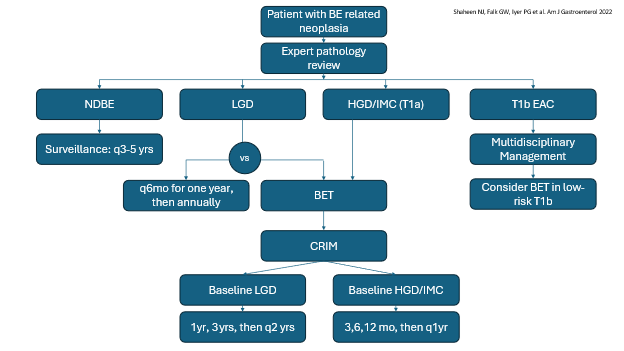
| LEGEND |
|---|
| BET | Barrett’s endoscopic therapy |
| CRIM | Complete remission of intestinal metaplasia |
| LGD | Low-grade dysplasia |
| HGD | High-grade dysplasia |
| IMC | Intramucosal cancer |
| NDBE | Nondysplastic Barrett’s esophagus |
REFERENCES
- Shaheen, Nicholas J. MD, MPH1; Falk, Gary W. MD, MS2; Iyer, Prasad G. MD, MS3; Souza, Rhonda F. MD4; Yadlapati, Rena H. MD, MHS (GRADE Methodologist)5; Sauer, Bryan G. MD, MSc (GRADE Methodologist)6; Wani, Sachin MD7. Diagnosis and Management of Barrett's Esophagus: An Updated ACG Guideline. The American Journal of Gastroenterology 117(4): p 559-587, April 2022. | DOI: 10.14309/ajg.0000000000001680
- Katz, Philip O. MD, MACG1; Dunbar, Kerry B. MD, PhD2,3; Schnoll-Sussman, Felice H. MD, FACG1; Greer, Katarina B. MD, MS, FACG4; Yadlapati, Rena MD, MSHS5; Spechler, Stuart Jon MD, FACG6,7. ACG Clinical Guideline for the Diagnosis and Management of Gastroesophageal Reflux Disease. The American Journal of Gastroenterology 117(1):p 27-56, January 2022. | DOI: 10.14309/ajg.0000000000001538
- Wang, Kenneth K. M.D.; Sampliner, Richard E. M.D. Updated Guidelines 2008 for the Diagnosis, Surveillance and Therapy of Barrett's Esophagus. American Journal of Gastroenterology 103(3):p 788-797, March 2008.
- Clermont M, Falk GW. Clinical Guidelines Update on the Diagnosis and Management of Barrett's Esophagus. Dig Dis Sci. 2018 Aug;63(8):2122-2128. doi: 10.1007/s10620-018-5070-z. PMID: 29671159.
- Tan MC, Kanthasamy KA, Yeh AG, Kil D, Pompeii L, Yu X, El-Serag HB, Thrift AP. Factors Associated With Recurrence of Barrett's Esophagus After Radiofrequency Ablation. Clin Gastroenterol Hepatol. 2019 Jan;17(1):65-72.e5. doi: 10.1016/j.cgh.2018.05.042. Epub 2018 Jun 11. PMID: 29902646.
Author

Sarel J. Myburgh, APRN, CNP, MS is a Nurse Practitioner Specialist with over ten years of diverse experiences in Rochester, Minnesota and affiliates with many hospitals in the Mayo Clinic Health System. He currently serves on the ASGE APP Committee.