
A 59 year old female with history of long-term alcohol use and current tobacco use was seen in the clinic with complaints of epigastric abdominal pain, bloating, and weight loss. She reported her pain radiated to the back and worsened with heavy meals. She also reported foul-smelling loose stools and sometimes noticing oil droplets in her stools. She had multiple hospitalizations for pain control over the year.
On examination, she is tender in the epigastric area and appears in mild distress. Labs demonstrate a normal serum lipase and mild elevation of alkaline phosphate (150 U/L). Computed tomography (CT) abdomen showed pancreatic parenchymal calcifications in the head and uncinate process. The pancreatic duct in the body and tail of pancreas was dilated to 12mm and intraductal calcifications were noted in the region of pancreatic head. MRI/MRCP confirmed dilatation of the main pancreatic duct dilation to 12 mm and a 10mm pancreatic duct calculus in the pancreatic head and chronic pancreatic volume loss.
What is the best appropriate next step for long-term management for the patient’s pain?
- Lateral Pancreaticojejuonsotymy (Puestow Procedure)
- ERCP with pancreas duct placement and stone extraction
- Endoscopic ultrasound guided celiac plexus neurolysis
- Conservative medical management
Show Answer
The correct answer is A, Lateral Pancreaticojejuonsotymy (Puestow Procedure).
Studies have shown that surgical drainage is more effective in long term pain control and lesser need for repeated intervention. Relieving the elevated pressure of the pancreas duct is critical for pain reduction. Although endoscopic therapy may provide short term relief, it rarely provides long term relief, and these patients will eventually need surgery. Endoscopic drainage may be considered for patients who are poor surgical candidates or those who prefer a less invasive option.5,6
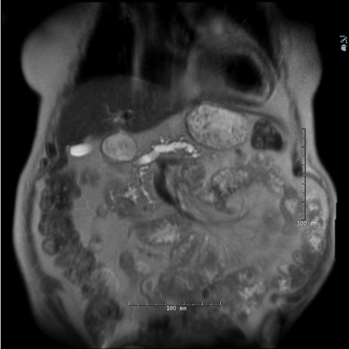
MRI noting pancreas calculus with pancreas ductal dilation.
Image from the library of Rush University Medical Center.
PRACTICE PEARLS
Epidemiology
- Incidence of Chronic pancreatitis (CP) is approximately 10 per 100,000 per year6
- More common in males and diagnosed in mid adulthood 3,4
- Alcohol remains the leading cause of cases in the United States2,3,4
- Cigarette smoking is an independent and dose dependent risk factor 2,3
- Other etiologies include genetic mutations (PRSS1, SPINK1, CFTR), autoimmune pancreatitis, ductal obstruction, metabolic causes, and idiopathic.2,3
Diagnosis
Chronic pancreatitis is a progressive irreversible inflammatory disorder of the pancreas with loss of the exocrine and endocrine function. It is based on a combination of clinical presentation, exposure to risk factors, pancreas functions test (direct and/or indirect), and cross-sectional imaging findings. 2
Clinical evaluation is critical in the diagnosis, with consideration of risk factors including alcohol use and tobacco use, history of recurrent acute pancreatitis, genetic predisposition, chronic abdominal pain, diabetes mellitus, and signs of pancreas exocrine insufficiency (steatorrhea, weight loss, and fat-soluble vitamin deficiencies). Note, advanced fibrosis and more than 90% function must be lost for exocrine and endocrine insufficiency to occur, so when patients develop these symptoms, it is usually always advanced disease 2,3
In patients with suspected CP, cross sectional imaging modalities including Computed tomography (CT) and magnetic resonance imaging (MRI). In cases of early disease, when CT and MRI are not conclusive, Endoscopic ultrasound (EUS) is more sensitive and can be helpful with diagnosis. The Rosemont criteria are used to make the diagnosis of chronic pancreatitis on EUS. Imaging finding would include pancreas atrophy, irregular or dilated pancreas duct, parenchymal calcifications, and parenchymal fibrosis.2,3,4
Diagnostic Tools
- History and Physical exam
- Imaging modalities including CT and MRI
- EUS if cross sectional findings are inconclusive
- Pancreas function test: fecal elastase, fecal fat, hemoglobin A1C, fat soluble vitamins levels
Pathogenesis and Pathology
The pathogenesis of chronic pancreatitis (CP) is complex and involves recurrent pancreatic injury leading to sustained inflammation. Damage to the acinar cells results in the release of inflammatory mediators and cytokines that activate pancreatic stellate cells, which then deposit extracellular matrix proteins and promote progressive fibrosis. The fibrotic process leads to acinar cell loss and architectural distortion of the pancreatic parenchyma as well as structural and functional changes in the pancreatic ducts. Pathological features changes include intrapancreatic calcifications, parenchymal atrophy, and ductal strictures or dilation. Progressive destruction of islet cells contributes to the development of both exocrine and endocrine pancreatic insufficiency.2,3,4
Management
- Management of CP requires a multidisciplinary approach
- Lifestyle modification including strict alcohol and smoking cessation2,4
- Pain control (non-opioid agents, neuromodulators, opioids, celiac plexus block)2,3
- Exocrine pancreas insufficiency: Pancreatic enzyme replacement therapy (PERT) for malabsorption and nutritional support with fat-soluble vitamin supplementation1
- Endocrine insufficiency with diabetes management (type 3c diabetes).1,4
- Endoscopic interventions (ERCP with pancreatic sphincterotomy, stone clearance, stricture dilation, and pancreatic duct stenting)2,3,4
- Surgical interventions include decompressive procedures (Puestow, Frey, and Beger procedures) 2,5,6
REFERENCES
- Bruni, A., Colecchia, L., Dell’Anna, G., Scalvini, D., Mandarino, F. V., Lisotti, A., Fuccio, L., Cecinato, P., Marasco, G., Donatelli, G., Barbara, G., & Eusebi, L. H. (2025). Nutritional management in chronic pancreatitis: From exocrine pancreatic insufficiency to precision therapy. Nutrients, 17(17), 2720. https://doi.org/10.3390/nu17172720
- Gardner, T. B., Adler, D. G., Forsmark, C. E., Sauer, B. G., Taylor, J. R., & Whitcomb, D. C. (2020). ACG clinical guideline: Chronic pancreatitis. The American Journal of Gastroenterology, 115(3), 322–339. https://doi.org/10.14309/ajg.0000000000000535
- Goosenberg, E., & Lappin, S. L. (2025, April 4). Chronic pancreatitis. In StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK482325/
- Hines, O. J., & Pandol, S. J. (2024). Management of chronic pancreatitis. BMJ (Clinical Research Ed.), 384, e070920. https://doi.org/10.1136/bmj-2023-070920
- Van Veldhuisen, C. L., Kempeneers, M. A., de Rijk, F. E. M., Bouwense, S. A., Bruno, M. J., Fockens, P., Poley, J. W., Ali, U. A., Bollen, T. L., Busch, O. R., van Duijvendijk, P., van Dullemen, H. M., van Eijck, C. H., Van Goor, H., Hadithi, M., Haveman, J. W., Keulemans, Y., Nieuwenhuijs, V. B., Poen, A. C., Voermans, R. P., … Dutch Pancreatitis Study Group (2025). Long-Term Outcomes of Early Surgery vs Endoscopy First in Chronic Pancreatitis: Follow-Up Analysis of the ESCAPE Randomized Clinical Trial. JAMA surgery, 160(2), 126–133. https://doi.org/10.1001/jamasurg.2024.5182
- Zhang, B., Liu, J., Bao, N., Xue, H., Feng, H., Lu, Z., Zhang, D., Sun, W., Shapaer, T., Zhao, Z., Shang, D., Bao, C., & Chen, Y. (2026). Global, regional, and national burden and future projections of pancreatitis: A Joinpoint, APC, and ARIMA modeling analysis. Clinical and experimental medicine, 26(1), 66. https://doi.org/10.1007/s10238-025-02023-0
Authors
Shaheen Patel DNP, APRN, AGACNP-BC, is an Advance Practice Provider for the Digestive Diseases and Nutrition Division at Rush University Medical Center and brings 10 years of experience in gastroenterology. She received her Bachelor of Nursing from at Loyola University Chicago and went on to earn her Doctorate of Nursing Practice from Rush University.

Ajaypal Singh, MD, is a gastroenterologist with expertise in interventional endoscopy. Dr. Singh is an Associate Professor in the Department of Medicine and serves as the Director of the Center for Interventional and Therapeutic Endoscopy (CITE) at Rush University Medical Center in Chicago, IL. His clinical interests include advanced tissue resection and interventional EUS. He is actively involved in teaching and is part of ASGE’s training and MSET committees.